Web Stories





Latest Blogs

Brain Fog: Meaning, Causes, Symptoms and Fixes
Have you ever felt mentally cloudy, like your brain is moving slower than usual, or like you are not as sharp as you normally are? That experience is often described as brain fog. It can be frustrating because it affects the basics: focusing at work, following conversations, remembering small details, and staying mentally present. Brain fog is not a medical diagnosis. It is a cluster of symptoms that can happen for many reasons, including poor sleep, stress, dehydration, hormonal shifts, nutrition gaps, illness recovery, or medication side effects. In this article, you will learn what brain fog means, what it feels like, the most common causes, practical ways to improve it, when to see a doctor, and what tests may help identify contributing factors. Medical note: This content is for general awareness and does not replace medical advice. If you have severe, sudden, or worrying symptoms, seek urgent medical care. What Is Brain Fog? Brain fog is a term people use to describe mental cloudiness with reduced clarity, focus, and memory, often paired with mental tiredness. It is usually a signal that something is affecting your brain’s day-to-day performance, such as poor sleep, stress, nutrition issues, hormonal changes, illness recovery, or certain medications. Brain fog in one sentence: Brain fog is the feeling of mental cloudiness that makes thinking, focusing, and remembering harder than usual. What Brain Fog Feels Like Brain fog often feels like your mind is “buffering,” like a slow phone that takes longer to respond. You know you should be able to think clearly, but everything feels delayed, fuzzy, or harder than usual. Common experiences include: Losing your train of thought mid-sentence Reading the same paragraph repeatedly without absorbing it Forgetting why you entered a room Struggling to find the right word during a conversation Feeling mentally tired even after small tasks, like replying to messages Some days it is mild and manageable. Other days it can make routine work feel surprisingly difficult. Symptoms of Brain Fog Common Symptoms Brain fog can look different from person to person, but these are some of the most common signs: Difficulty focusing or paying attention Forgetfulness and short-term memory slips (names, dates, small tasks) Slow thinking and slower reaction time Word-finding difficulty (you know what you want to say, but the word does not come) Mental fatigue, feeling “spaced out” or not fully present Trouble multitasking or learning new information A quick self-check: if you notice several of these symptoms regularly for days or weeks, it is worth looking for patterns and triggers rather than brushing it off as “just being busy.” Causes of Brain Fog Brain fog is often caused by more than one factor. That is why it helps to start with the most common triggers first and work step by step. Lifestyle Causes These are some of the biggest and most fixable contributors: Poor sleep or an irregular sleep schedule Chronic stress and burnout Dehydration, especially if you rely heavily on caffeine Skipping meals or eating mostly sugary and refined foods that cause energy crashes Too much alcohol, which can affect sleep quality and attention Overload, meaning too much screen time, too many tasks, and not enough breaks If brain fog started during a busy period, lifestyle factors are often a major piece of the puzzle. Hormonal Changes Hormones influence sleep, mood, and mental performance. Brain fog may occur with: Menstrual cycle changes Pregnancy and the postpartum period Perimenopause and menopause If symptoms seem to follow a cycle or life phase, tracking timing can help you and your clinician understand what is going on. Mental Health and Emotional Load Your brain struggles to focus when it is under emotional pressure. Anxiety and low mood can reduce attention, motivation, and working memory High stress can worsen sleep and concentration This does not mean symptoms are imagined. It means brain fog can be part of how your mind and body respond to prolonged strain. Medical Contributors That Are Often Treatable Brain fog does not always mean something serious. Often there are common and treatable contributors, such as: Thyroid imbalance Low iron or anaemia Vitamin B12 deficiency Blood sugar issues, including diabetes or low blood sugar episodes Vitamin D deficiency, which is commonly checked in fatigue workups Only a clinician can confirm whether these apply to you, but it helps to know these are common possibilities. Infections and Recovery Periods Brain fog can occur during recovery, especially after illness: Brain fog after a viral illness is common and often temporary Long COVID is a recognised trigger for ongoing concentration and fatigue issues in some people If your brain fog began after an infection, pacing yourself and giving your body time to recover can matter as much as rest. Chronic Conditions Sometimes Linked With Brain Fog Brain fog can be reported alongside some longer-term conditions, including: Autoimmune conditions Chronic fatigue-related syndromes Neurological conditions (in a general sense) This does not mean brain fog automatically points to these conditions. It simply means brain fog can occur in many contexts. Medications and Substances Some medicines can cause drowsiness, slowed thinking, or attention problems. Alcohol and other substances can also worsen focus and sleep quality. Safety note: do not stop medicines without medical advice. If symptoms began after starting a new medication, discuss it with your clinician. A helpful way to think about it: brain fog often comes from a combination, like stress plus poor sleep plus low iron, rather than one single cause. Brain Fog, Dementia, and Delirium: Key Differences It is common to worry that brain fog might be dementia. Most of the time, it is not, but it is still important to understand how they differ. Brain fog is usually fluctuating and often linked to triggers like sleep loss, stress, illness recovery, dehydration, or lifestyle patterns. Dementia is generally progressive over time and increasingly affects daily functioning. Delirium is sudden confusion and is a medical emergency. It may involve disorientation, severe confusion, or changes in alertness. If your symptoms are worsening quickly, affecting safety, or paired with red flag symptoms, seek urgent medical care. How to Clear Brain Fog The most effective approach is to reduce what is draining your brain and build habits that support steady energy, sleep quality, and recovery. You do not need to do everything. Start with a few changes you can maintain. Quick Improvements in the Next 24 to 72 Hours These steps can help quickly, especially when lifestyle factors play a role: Hydrate consistently and eat regular meals Reduce late caffeine and alcohol Take a short walk or do light exercise Take 10-minute breaks with no screens between mentally demanding tasks Use a simple to-do list and do one task at a time Even small changes can improve mental clarity more than you expect. Resetting Sleep for Better Mental Clarity Sleep is one of the biggest drivers of focus and memory. Keep consistent sleep and wake times, even on weekends Get morning sunlight exposure to support your body clock Set a screen cut-off time before bed Keep the bedroom dark, quiet, and cool If you wake up tired often, snore heavily, or feel unusually sleepy in the day, speak with a clinician. Sleep problems are common and treatable. Food and Nutrition Habits That Support Focus You do not need a strict diet. You need steady fuel. Aim for protein with breakfast to reduce energy crashes Choose balanced meals to avoid glucose spikes and crashes Include iron and B12 rich foods, without expecting overnight results If you are vegetarian or vegan, be mindful of B12 intake and consider discussing testing if symptoms persist If you suspect certain foods make symptoms worse, a simple food and symptom diary can help identify patterns Stress Management That Fits Real Life Stress is part of life, but you can reduce its mental cost. Try a 5-minute breathing routine once or twice a day Use movement breaks to reset attention Set boundaries around workload where possible Build recovery time into the day, not just the weekend If anxiety or low mood is persistent, speaking with a mental health professional can help. Better mental health often improves sleep and focus. Focus Strategies for Busy Days When you must perform, reduce friction. Single-task whenever possible Use timed focus blocks (for example 25 minutes focus, 5 minutes break) Reduce distractions and work in a quieter space Write things down, use reminders, and keep simple routines Brain fog often worsens when you try to multitask. One task at a time usually works better. A Simple 2-Week Plan If you want a clear plan, try this: Week 1 Improve sleep timing as much as possible Increase hydration Add a daily walk, even if it is 15 to 20 minutes Week 2 Keep sleep steady Shift meals toward balanced plates and reduce high sugar snacks Add a short daily stress routine Cut back alcohol Track symptoms briefly in a note app: what improves, what worsens, and when you feel best. This can reveal triggers you did not notice before. When to See a Doctor See a Clinician If Brain fog lasts more than 2 to 3 weeks It is getting worse It affects work, driving, or daily tasks You have new symptoms like significant mood changes, weakness, or persistent headaches Seek Urgent Medical Care If You Notice Red Flags Sudden weakness or numbness, especially one-sided Facial drooping Trouble speaking or understanding speech Severe sudden headache Seizure Fainting or severe confusion Sudden vision loss Severe imbalance If you are in India, you can call 112 for emergency assistance. How Brain Fog Is Evaluated History and Basic Examination Clinicians usually start with questions about: Sleep, stress, diet, hydration Recent illness or infection recovery Medicines and supplements Mood, workload, burnout, and life changes Other symptoms like headaches, dizziness, weakness, or appetite changes A basic neurological and general assessment may check coordination, reflexes, attention, and overall health. Lab Tests That May Help Identify Contributing Factors Your doctor may recommend tests to rule out common contributors, such as: Complete Blood Count (CBC) Iron studies (if clinically indicated) Thyroid Profile (TSH, T3, T4) Vitamin B12 Vitamin D Blood glucose or HbA1c Electrolytes (Sodium, Potassium, Calcium, Magnesium) CRP (when inflammation is suspected) If your clinician advises tests, you can book them with Metropolis and review the results with your doctor for interpretation and next steps. Imaging and Diagnostic Tests to Identify Brain Fog There is no single scan or machine test that “detects brain fog.” Instead, imaging and other diagnostic tests are used selectively when a clinician wants to rule out specific neurological causes or investigate concerning symptoms. A doctor may consider additional testing if brain fog is persistent, worsening, affects safety, or is accompanied by symptoms like severe headaches, fainting, seizures, weakness, numbness, speech changes, vision changes, or changes in alertness. Common tests that may be recommended in certain situations include: CT or MRI brain: These scans may be used when there are red flags, a history of head injury, new neurological signs, or concern for causes such as stroke, bleeding, inflammation, or structural changes. EEG: This test measures brain electrical activity and may be advised if seizures are suspected or if there are episodes of unexplained confusion or altered awareness. Sleep testing: If symptoms include loud snoring, pauses in breathing during sleep, or marked daytime sleepiness, a clinician may evaluate for sleep disorders such as obstructive sleep apnea, which can strongly affect attention and memory. Cognitive screening or neuropsychological testing: If memory or thinking problems are prominent, structured assessments can help clarify which domains are affected and guide next steps. Other targeted tests: Depending on the pattern of symptoms, a clinician may advise additional evaluations related to balance, vision, hearing, or autonomic function. In many people, lifestyle factors and common medical contributors are identified through history, examination, and blood tests. Imaging is typically reserved for situations where the symptom pattern suggests a need to rule out neurological disease. Medical Treatment for Brain Fog Because brain fog is a symptom cluster rather than a single diagnosis, medical treatment depends on the underlying cause. The goal is usually to identify and address what is driving the fog, then support recovery with practical measures. A clinician may consider medical treatment approaches such as: Reviewing medications: If brain fog started after a new medicine or a dose change, a doctor may adjust timing, switch to an alternative, or reduce dose when clinically appropriate. Treating thyroid imbalance: If thyroid hormones are outside the healthy range, treatment can improve fatigue, attention, and mental clarity over time. Correcting anaemia or iron deficiency: If testing suggests low iron or anaemia, treatment may include diet changes and iron therapy under medical guidance. Treating vitamin B12 deficiency: B12 deficiency is a treatable cause of fatigue and cognitive symptoms. Treatment may involve oral supplements or injections, depending on the cause and severity. Managing blood sugar issues: If glucose fluctuations or diabetes are contributing, a treatment plan may include dietary adjustments, activity, and medications as advised. Addressing sleep disorders: Conditions like sleep apnea can cause significant daytime fog. Treatment can meaningfully improve attention, mood, and energy. Supporting mental health: If anxiety or depression is contributing, treatment may involve therapy, structured lifestyle changes, and sometimes medication, guided by a clinician. Treating infections or inflammatory causes: If brain fog follows an illness and symptoms persist or worsen, medical evaluation helps rule out complications and guide appropriate treatment. If brain fog is severe, sudden, or paired with neurological symptoms, treatment is urgent and focused on ruling out time-sensitive conditions such as stroke or serious infection. Can Supplements Help With Brain Fog? Supplements can help in specific situations, but they are not a universal fix. In general, supplements are most useful when they correct a confirmed deficiency or support a clinician-guided plan. Situations where supplements may be considered include: Vitamin B12: Particularly relevant for people with low levels, vegetarian or vegan diets, or absorption issues. Iron: Helpful only when iron deficiency is confirmed, since unnecessary iron can be harmful. Vitamin D: Sometimes used when low levels are found during fatigue and wellness evaluation. Omega-3 fats: Often discussed for brain health, though effects on day-to-day fog can vary by person. Practical guidance: Test first when possible, especially for B12, iron, and vitamin D. Avoid stacking multiple supplements at high doses. Tell your clinician about supplements, especially if you take blood thinners, thyroid medicines, diabetes medicines, or anti-seizure medicines. Be cautious with products marketed as “brain boosters” or “nootropics.” Many have limited evidence, and some can worsen sleep, anxiety, or heart rate. If you choose to try a supplement, a simple approach is best: one change at a time, for a defined period, with attention to sleep, hydration, and diet. Can Brain Fog Be Prevented? You cannot prevent every episode, but you can reduce the chances and severity. Maintain consistent sleep Eat regular balanced meals and stay hydrated Manage stress and build recovery time Move daily, even lightly Review medications with your clinician if symptoms start after a new prescription Keep chronic conditions monitored and follow medical advice Frequently Asked Questions What is brain fog meaning in simple words? Brain fog means feeling mentally cloudy, with difficulty focusing, thinking clearly, or remembering things. Is brain fog a disease? No. Brain fog is not a disease. It is a group of symptoms that can have many causes. What are the most common brain fog symptoms? Poor focus, forgetfulness, slow thinking, word-finding difficulty, mental fatigue, and trouble multitasking are common. What causes brain fog in daily life? Poor sleep, stress, dehydration, irregular meals, sugary foods, alcohol, and mental overload are common triggers. Can stress and poor sleep really cause brain fog? Yes. Poor sleep affects attention and memory, and stress increases mental fatigue and reduces clarity. How long does brain fog last? It varies. It can last days or weeks. If it persists beyond 2 to 3 weeks or worsens, speak with a clinician. Brain fog vs dementia: what is the difference? Brain fog often fluctuates and may improve when triggers are addressed. Dementia is generally progressive and affects daily functioning over time. What helps brain fog fast? Hydration, regular meals, improved sleep timing, reducing late caffeine and alcohol, short walks, and screen-free breaks can help within 24 to 72 hours for many people. When should I see a doctor for brain fog? If it lasts more than 2 to 3 weeks, worsens, affects daily tasks or safety, or comes with new symptoms like weakness or persistent headaches. Which blood tests can help find causes of brain fog? Common tests include CBC, thyroid profile, vitamin B12, vitamin D, glucose or HbA1c, electrolytes, and sometimes iron studies and CRP based on symptoms.

Brain MRI: What It Detects, Procedure and Report Terms
A head MRI, also called a brain MRI, is one of the most common scans used to look closely at the brain and nearby structures. People often search for “MRI head” when they have symptoms like headaches that will not settle, dizziness, seizures, changes in vision, memory concerns, or unexplained weakness. The idea of lying inside a scanner can feel intimidating, especially if you have never had imaging before. The good news is that a head MRI is painless and does not use radiation. It uses a strong magnet and radio waves to create detailed pictures of soft tissues, which helps clinicians understand what is happening and what to do next. This guide explains what a head MRI can detect, how to prepare, what happens during the scan, what “contrast” means, and how to make sense of common MRI report terms. Medical note: This article is for general education and does not replace medical advice. Always discuss your results and next steps with your clinician. What Is a Brain MRI? A head MRI (Magnetic Resonance Imaging) is a scan that creates detailed images of the brain and surrounding tissues using a powerful magnet, radio waves, and a computer. It is often called a brain MRI, and in day-to-day practice the terms are usually used interchangeably. Unlike X-rays and CT scans, an MRI does not use ionizing radiation. That makes it a preferred option in many situations where detailed soft-tissue imaging is important. What Can a Brain MRI Detect? A head MRI can help clinicians look for changes in the brain’s structure, blood flow patterns, and surrounding tissues. It may be used to detect or assess: Stroke-related changes, including early stroke changes in certain MRI sequences Bleeding, swelling, or fluid build-up Tumours or other masses Inflammation and some infections Conditions that affect the brain’s white matter, including demyelinating disorders such as multiple sclerosis Structural abnormalities, including developmental changes Pituitary gland issues and nearby structures (in dedicated pituitary MRI studies) Causes of seizures, depending on the clinical context Inner ear and eye-related structures (in some protocols), plus cranial nerves A head MRI can also be used to monitor known conditions over time, such as changes after treatment, stability of lesions, or follow-up for ongoing symptoms. When Is a Head MRI Recommended? A clinician may suggest an MRI head scan when symptoms need deeper evaluation, for example: Persistent or unusual headaches, especially with additional symptoms Seizures or unexplained fainting episodes Dizziness or balance problems that are ongoing or severe Sudden changes in vision, hearing, or speech New weakness, numbness, or coordination changes Memory or thinking changes that need further assessment Symptoms after head injury, depending on the situation and timing Hormonal symptoms when pituitary involvement is suspected In emergencies, CT is sometimes used first because it is faster and widely available. MRI is often used next, or when more detail is needed. Head MRI vs CT Scan: What Is the Difference? Both CT and MRI can image the brain, but they do it differently. CT scans use X-rays. They are fast and helpful in many emergency settings. MRI scans use magnets and radio waves. They usually take longer but provide more detailed views of brain soft tissue. Your clinician chooses the test based on symptoms, urgency, and the question they are trying to answer. Head MRI With Contrast: What It Means Some brain MRI exams are done “with contrast.” This means a contrast agent, commonly a gadolinium-based dye, is injected into a vein during the scan to help certain tissues show up more clearly. Contrast can improve the visibility of: Some tumours and patterns of inflammation Certain infections Blood vessels and areas of abnormal blood supply Specific changes after stroke (depending on timing and protocol) Not every MRI needs contrast. Many are done without it, and your clinician or radiology team decides based on your symptoms and the best imaging approach. Important safety note: If you have kidney disease, have had a previous reaction to contrast, or are pregnant or might be pregnant, tell your clinician and the MRI staff before the scan. They can decide what is safest for you. How to Prepare for a Head MRI Preparation is usually simple, but the safety checklist matters. Before You Arrive Follow instructions from the imaging centre, especially if contrast is planned. Some centres may ask you to avoid eating for a few hours beforehand. Take your regular medications unless your clinician advises otherwise. Wear comfortable clothing. You may be asked to change into a gown. Remove Metal and Mention Implants MRI magnets are strong, so you must remove metal items such as: Jewellery, watches, hairpins, and belts Credit cards and phones (they can be damaged) Removable dental items, hearing aids, and some wearable devices Tell the team if you have any implants or metal in your body, such as: Pacemaker or implanted defibrillator Cochlear implant Aneurysm clip Metal fragments from past injuries or work exposures Implanted pumps or stimulators Some types of surgical hardware Many implants are MRI-safe or MRI-conditional, but the team needs details to confirm safety. If You Have Claustrophobia If enclosed spaces make you anxious, you are not alone. Options may include: A mild sedative prescribed in advance A wide-bore or open MRI machine if available Practical tips like closing your eyes, focusing on breathing, or listening to music through headphones If sedation is used, you may need someone to accompany you home. What Happens During the Scan? A head MRI is usually painless, but it requires stillness and patience. Step by Step You lie on a table that slides into the MRI scanner. A “head coil” is positioned around your head, like a helmet frame, to help capture clear images. The scan begins. You will hear loud tapping, knocking, or humming sounds in short sequences. Earplugs or headphones are provided. You must stay very still. Even small movements can blur images. If contrast is needed, an IV is used to inject it during the scan. How Long It Takes Most brain MRI scans take about 30 to 60 minutes, sometimes longer depending on the protocol and whether contrast is used. What You Might Feel No pain from the scan itself The table may feel firm or cool (you can request a blanket in many centres) Some people feel warm in the scanned area If contrast is given, a brief cool sensation in the arm is common, and some people notice a temporary metallic taste After the Scan: What to Expect If you did not receive sedation, you can usually: Eat and drink normally Resume normal activities right away If you received a sedative, you may need: A short recovery period Someone to drive you home Instructions about resting for the remainder of the day A radiologist reviews the images and sends a report to the clinician who ordered the scan. The timeline varies, but many reports are available within a day or two. Common Head MRI Report Terms and What They Usually Mean MRI reports are written for clinicians, so the wording can sound alarming even when findings are minor or expected. Below are common terms and plain-language explanations. These are general explanations, not a diagnosis. “No Acute Intracranial Abnormality” This often means there is no clear evidence of a recent major problem, such as a large bleed, a significant mass, or a major acute stroke pattern on the sequences reviewed. “Incidental Finding” An incidental finding is something seen on the scan that was not the main reason for the MRI. Many incidental findings are harmless, but some require monitoring. “Lesion” A lesion is a general word for an area that looks different from surrounding tissue. It does not automatically mean cancer. Context and pattern matter. “White Matter Changes” or “White Matter Hyperintensities” White matter refers to the brain’s communication pathways. “Changes” can be seen for many reasons, including age-related changes, migraine-associated patterns in some people, vascular risk factors, and inflammatory conditions. The significance depends on your age, symptoms, and health history. “FLAIR Hyperintensity” FLAIR is a type of MRI sequence. A “hyperintensity” means an area appears brighter on that sequence. It is a description, not a diagnosis. “Restricted Diffusion” or “DWI” Diffusion-weighted imaging (DWI) looks at how water moves in tissue. “Restricted diffusion” can be seen in certain acute processes such as early stroke, but it can also appear in other conditions. It must be interpreted with the full scan and your symptoms. “Enhancement” If contrast is used, “enhancement” means an area takes up contrast and appears brighter. This can occur with inflammation, infection, some tumours, and other processes. The pattern of enhancement is important. “Edema” Edema means swelling, often due to fluid in tissue. MRI can show edema around tumours, after injury, or with inflammation. “Mass Effect” and “Midline Shift” “Mass effect” means something is pressing on nearby structures. “Midline shift” means pressure has moved structures away from the centre line. These terms are taken seriously and usually require urgent clinical correlation. “Atrophy” or “Volume Loss” Atrophy refers to reduced brain volume. Some degree can occur with aging. The report often describes where it is seen and whether it appears more than expected for age. “Ventricles” Ventricles are fluid-filled spaces in the brain. The report may describe them as normal, prominent, enlarged, or compressed, depending on what is seen. “Sinus Mucosal Thickening” This usually refers to inflammation in the sinus lining. It can be related to sinus congestion and is commonly incidental on head imaging. “Artifact” An artifact is image distortion, often from movement, dental work, or metal. It does not mean disease, it means image quality was affected. Tip: If a report worries you, ask your clinician two simple questions: What findings matter for my symptoms? What happens next, if anything? MRI Safety and Risks A head MRI is considered very safe for most people, but there are a few important safety points: The magnet can interact with certain implants or metal fragments, so screening is essential. Contrast reactions are uncommon, and serious allergic reactions are rare. Gadolinium contrast is handled carefully in people with significant kidney disease. Pregnancy considerations vary by trimester and urgency, so always inform your clinician if you are pregnant or might be pregnant. The radiology team’s screening questions may feel repetitive, but they are there to keep you safe. Frequently Asked Questions Is a head MRI the same as a brain MRI? In most cases, yes. Both terms are commonly used for the same scan of the brain and structures in the head. Some protocols focus on specific areas, such as the pituitary gland. Does an MRI head scan use radiation? No. MRI uses magnets and radio waves, not ionizing radiation. How long does a brain MRI take? Commonly 30 to 60 minutes, sometimes longer depending on the protocol and whether contrast is used. What is contrast and do I need it? Contrast is a dye injected through an IV to improve visibility of certain tissues. Not all MRIs need it. The decision depends on symptoms and what the clinician is looking for. What if I have claustrophobia? Many centres offer options such as headphones, mirrors, calming techniques, wide-bore scanners, or sedation when appropriate. Tell the team in advance. Can I eat before a head MRI? Often yes, but instructions can vary, especially if contrast or sedation is planned. Follow the imaging centre’s guidance. When will I get results? A radiologist reviews the scan and sends a report to your clinician. Many reports are available within a day or two, but timelines vary. What should I do if my MRI report has scary terms? Do not panic based on wording alone. Reports use technical descriptions. Discuss what the findings mean in your situation with your clinician.
Brainstem: Functions, Parts, and Common Conditions
Your heartbeat stays steady, your breathing adjusts to what you are doing, you swallow without thinking, you keep your balance while walking, and you stay alert enough to respond to the world. Most of this happens automatically, without you giving a single instruction. A major reason is the brainstem. The brainstem is a small but vital structure that connects the brain to the spinal cord and helps run many core functions that keep you alive and functioning. In this guide, you will learn what the brainstem is, where it sits, its three main parts, what it controls, which symptoms matter, and how doctors check it. Medical note: This content is for education only and is not a substitute for medical advice. What Is The Brainstem? The brainstem is the stalk-like connection between the brain and the spinal cord. It keeps essential functions running automatically and acts as a major signal highway between the brain and the rest of the body. Brainstem in one sentence: The brainstem is the body’s built-in control and relay centre that keeps life-support functions running while carrying messages between the brain and spinal cord. Where Is The Brainstem Located And Why Is It So Important? The brainstem sits at the base of the brain, in front of the cerebellum, and continues downward into the spinal cord. It is small compared with the rest of the brain, but it is packed with critical pathways and control centres. Why it matters is simple: the brainstem helps regulate core survival functions like breathing, heart rate, and blood pressure. It also supports alertness, basic reflexes that protect you (like coughing and swallowing), and constant communication between the brain and body. Because so many important functions pass through such a compact area, even small problems in the brainstem can cause noticeable symptoms. Visual idea: A simple labelled diagram showing the cerebrum, cerebellum, brainstem, and spinal cord, with arrows indicating two-way signal flow. Brain Stem Parts (Anatomy) Explained The brainstem has three main parts: the midbrain, pons, and medulla oblongata. Midbrain (Top Portion) The midbrain sits at the top of the brainstem. It plays a key role in: Eye movement control Visual and hearing reflexes Support for motor control Sleep-wake regulation and attention-related processes If you think of the brainstem as a busy junction, the midbrain is one of the upper control hubs where movement and sensory reflexes meet. Pons (Middle Portion) The pons is the middle section. It helps: Relay signals between the cerebrum and cerebellum Regulate breathing patterns Support sleep and arousal Coordinate facial sensation and movement Support hearing and balance pathways The pons is also a major “bridge” for communication, which is exactly what its name suggests. Medulla Oblongata (Lowest Portion) The medulla oblongata is the lowest part of the brainstem and merges into the spinal cord. It helps regulate: Breathing Heart rate Blood pressure Swallowing Coughing and vomiting reflexes Because these functions are so fundamental, the medulla is often described as one of the most essential control centres in the nervous system. Think of the brainstem as a connector plus an autopilot: it connects the brain to the body while automatically running vital functions you should not have to think about. Brain Stem Function (What It Controls) The brainstem’s job can be understood in four simple buckets: life support, alertness, relay, and reflexes. Life Support Functions You Do Not Think About The brainstem helps regulate functions that run continuously: Breathing rhythm and airway protection: It supports the breathing pattern and protective actions like coughing if something “goes down the wrong way.” Heart rate and blood pressure regulation: It helps keep circulation stable, especially as you rest, stand, exercise, or feel stress. Basic autonomic balance support: It contributes to the automatic side of the nervous system that keeps internal systems steady. These are not “on or off” switches. They are constant adjustments, minute by minute, that keep your body in balance. Alertness, Consciousness, And Sleep-Wake Control A network within the brainstem called the reticular formation helps regulate wakefulness, attention, and the sleep-wake cycle. In plain language, it is one of the systems that helps your brain stay “online” enough to be aware of your surroundings and to shift between being alert and being asleep. When this system is affected, people may feel unusually drowsy, less responsive, or mentally slowed, depending on the cause and severity. The Brain’s Main Relay Station The brainstem is a two-way highway: It sends motor commands down from the brain to the body. It brings sensory information up from the body to the brain. Messages travel through the brainstem all day, every day, whether you are moving, speaking, swallowing, or just maintaining posture and balance. Brainstem Reflexes That Protect You Many protective reflexes are coordinated through the brainstem, including: Pupillary light reflex: pupils adjust to bright or dim light Swallow and gag reflex: helps protect the airway and move food safely Cough and sneeze reflexes: help clear irritants Eye stabilization during head movement (vestibulo-ocular reflex): helps keep vision steady when you move These reflexes are fast and automatic, and they exist to protect you and keep basic functions stable. Brainstem And Cranial Nerves (What The Brainstem Helps You Do) Cranial nerves are like specialized “wires” that control and carry information for the face, eyes, hearing, balance, swallowing, voice, and more. Many of the control centres for these nerves sit in or connect through the brainstem, which is why brainstem health is closely tied to things like eye movement, facial strength, speech clarity, and swallowing. Quick Map By Region Midbrain: Key control for eye movements and visual reflexes Pons: Facial movement and sensation, hearing and balance support Medulla: Swallowing and voice support, heart and breathing regulation support Here is a simple way to connect function to everyday experience: Function Area What It Helps With What Someone Might Notice If Affected Eye movement control Coordinated gaze, steady vision Double vision, trouble tracking, unusual eye movement symptoms Facial sensation and movement Facial expressions, sensation Facial numbness, drooping, changes in expression Swallowing and voice Safe swallowing, clear speech Choking, coughing while eating, hoarse voice, slurred speech Balance pathways Stable posture and coordination Dizziness, vertigo, unsteady walking Symptoms can overlap with many other conditions, so this table is not for self-diagnosis. It is simply a way to understand why the brainstem can affect multiple functions at once. Common Conditions That Can Affect The Brainstem Many different issues can involve the brainstem. Most people never have a brainstem condition, but it helps to understand the broad categories. Vascular events: Reduced blood flow or bleeding can affect brainstem function. Head injury and trauma: Impact injuries can affect brain tissue directly or through swelling. Infections and inflammation: Some infections can involve the brain or the tissues around it, leading to brainstem-related symptoms. Growths or pressure effects: Masses, swelling, or fluid-related pressure can crowd nearby structures. Demyelinating or nerve-signal conditions: Some conditions disrupt how nerve signals travel. Structural or congenital issues: Certain structural patterns can crowd the lower part of the brain, sometimes affecting brainstem and nearby pathways. Metabolic issues: Severe imbalances, such as significant electrolyte disturbances, can affect brain function and alertness. A key point: symptoms vary widely because many pathways pass through a small space. The same symptom, like dizziness or slurred speech, can also come from causes outside the brainstem. That is why clinical evaluation matters. Signs And Symptoms Linked To Brainstem Involvement Symptoms People Commonly Notice People may notice one or more of these symptoms when brainstem pathways are involved: Dizziness or vertigo Double vision or unusual eye movement symptoms Slurred speech Swallowing difficulty Balance and coordination problems Weakness or numbness Changes in alertness or unusual sleepiness These symptoms can have many explanations, including non-brainstem causes. What matters most is the pattern, severity, and timing. Red Flags That Need Urgent Medical Care Seek urgent medical care if you or someone else has: Sudden one-sided weakness or numbness Facial drooping Trouble speaking or understanding speech Sudden severe headache Fainting, severe confusion, or reduced consciousness New seizure Sudden vision loss Severe imbalance that starts suddenly Breathing difficulty or repeated choking If symptoms begin suddenly or worsen quickly, do not wait it out. Sudden neurological symptoms should be treated as time-sensitive. How Doctors Check The Brainstem History And Basic Examination A clinician usually starts with a careful history and exam. This often includes: Symptom timing (sudden vs gradual) Triggers and what makes symptoms better or worse Current medications and recent medication changes Recent illness or injury Relevant medical history such as blood pressure, blood sugar issues, or prior neurological concerns A focused neurological exam may include checks of: Eye movements and pupil response Facial movements Speech clarity Swallowing and voice quality Coordination and balance Strength and sensation Reflexes This exam helps narrow down which pathways might be involved and what testing is most useful. Imaging Tests (When Clinically Advised) Imaging is not always needed, but it can be crucial depending on symptoms. MRI: A detailed soft-tissue scan that can evaluate brain structures closely, including the brainstem. It is often used when doctors need high-detail information. CT: A faster scan often used in emergencies, especially when speed matters. The choice depends on the situation, symptoms, and what the clinician is trying to rule out. Other Tests That May Help In Specific Cases Depending on symptoms and clinical judgement, a doctor may consider: Hearing and balance related testing: when dizziness, vertigo, or hearing changes are prominent Evoked potential testing: when a clinician wants information about how certain nerve pathways are conducting signals Swallow evaluation: when choking, coughing during meals, or swallowing difficulty is present Blood Tests That May Help Identify Contributing Factors Your clinician may recommend tests to rule out common contributors, especially when symptoms like dizziness, fatigue, or mental fog overlap with broader health issues: Complete Blood Count (CBC) Electrolytes (sodium, potassium, calcium, magnesium) Blood glucose or HbA1c Thyroid profile (TSH, T3, T4) Vitamin B12 Inflammation marker such as CRP (when relevant) If your clinician recommends lab tests, you can book them with Metropolis Healthcare and review the results with your doctor to understand what they mean in your specific context. Brainstem Health Basics You cannot “exercise” the brainstem directly, but you can reduce risks and support overall nervous system health: Wear helmets and seatbelts, and prevent falls: many serious neurological injuries are preventable. Manage blood pressure, blood sugar, and cholesterol if advised: vascular health supports brain health. Support sleep and stress recovery: steady sleep and stress management support attention, balance, and overall nervous system function. Medication safety matters: do not stop or change medicines without medical guidance. If symptoms started after a new medication, tell your clinician. When symptoms change suddenly, do not wait: sudden neurological symptoms should be assessed urgently. FAQs What Is The Brainstem And What Does It Do? The brainstem connects the brain to the spinal cord. It helps regulate essential automatic functions like breathing, heart rate, blood pressure, alertness, and protective reflexes, while also carrying messages between the brain and body. What Are The Three Parts Of The Brainstem? The brainstem has three main parts: the midbrain, pons, and medulla oblongata. What Is The Function Of The Medulla Oblongata? The medulla supports vital functions such as breathing, heart rate, blood pressure regulation, and protective reflexes like swallowing and coughing. It also merges into the spinal cord. How Does The Brainstem Control Breathing And Heart Rate? The brainstem contains control centres that continuously adjust breathing rhythm and heart activity based on the body’s needs, such as rest, movement, and stress. Which Cranial Nerves Are Connected To The Brainstem? Many cranial nerve control centres sit in the brainstem. These nerves are involved in eye movements, facial sensation and movement, hearing and balance, swallowing, and voice. What Are Common Brainstem Reflexes? Common brainstem reflexes include pupil response to light, swallowing and gag reflexes, coughing and sneezing reflexes, and eye stabilization when the head moves. What Symptoms Could Suggest A Brainstem Problem? Possible symptoms include dizziness or vertigo, double vision, slurred speech, swallowing difficulty, imbalance, weakness or numbness, and unusual sleepiness. These symptoms can also come from other causes, so medical evaluation is important. Can A Brainstem Injury Be Treated Or Improved? Treatment depends on the cause. Some brainstem problems improve with prompt care, rehabilitation, and targeted treatment, while others require urgent intervention. Early assessment often improves outcomes. Why Is MRI Used To Look At The Brainstem? MRI provides detailed images of soft tissues and can help evaluate brain structures closely, including the brainstem. Doctors choose MRI or CT based on urgency, symptoms, and clinical goals. What Is The Difference Between Coma, Brain Death, And Brainstem Function Loss? Coma refers to a state of unresponsiveness where a person is not awake and not aware. Brain death is an irreversible loss of brain function, which includes loss of brainstem function. Brainstem function loss is particularly critical because the brainstem supports breathing and other life-sustaining reflexes. These are complex medical determinations made by trained clinicians using established protocols.
Blood-Brain Barrier: What It Is And Why It Matters
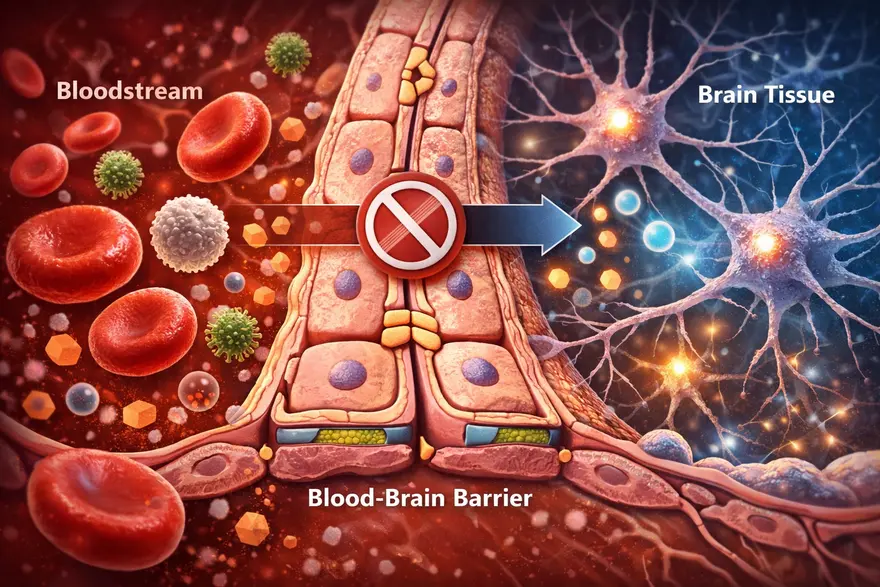
Your brain needs constant fuel from your blood, like oxygen, glucose, and other nutrients. But it also needs protection from germs, toxins, and sudden chemical shifts that could disrupt delicate brain signalling. That is where the blood-brain barrier (BBB) comes in. The BBB is a specialized “gatekeeper” built into the small blood vessels of the brain. It carefully controls what can enter and leave brain tissue, helping keep the brain’s internal environment stable. In this article, you will learn what the blood-brain barrier is, how it works, what can (and cannot) cross it, what happens when it is disrupted, and why it matters for neurological conditions and medicines. Medical note: This is educational information, not a substitute for medical advice. What Is The Blood-Brain Barrier? The blood-brain barrier is a highly selective filter formed by specialized cells lining the brain’s tiny blood vessels. It protects the brain by allowing essential nutrients in while blocking many harmful substances, germs, and toxins. Blood-brain barrier in one sentence: It is the brain’s security system, a tight, selective lining of blood vessels that controls what reaches brain tissue. Why Is The Blood-Brain Barrier So Important? The brain is extremely sensitive to changes in its chemical environment. Even small shifts in salts (electrolytes), hormones, or inflammatory molecules can affect how neurons communicate. The BBB helps by: Protecting the brain from pathogens and circulating toxins Maintaining stability (brain “homeostasis”) so neurons can function normally Controlling immune access, limiting unnecessary inflammation in brain tissue Influencing treatment, because many medicines cannot easily cross it In short, the BBB is one reason your brain can stay stable and functional even while your bloodstream changes with meals, exercise, stress, or illness. Blood-Brain Barrier Structure: What It’s Made Of The BBB is not one single wall. It is a set of structures working together in what scientists often call the neurovascular unit. The key components include: Endothelial Cells With Tight Junctions (The “Sealed Lining”) Brain capillaries are lined by endothelial cells that are packed unusually tight. The tight junctions between them act like sealant, preventing many substances from slipping between cells. Basement Membrane (The Support Layer) A thin structural layer supports the vessel wall and helps organize the barrier’s architecture. Pericytes (Stability And Regulation) Pericytes wrap around capillaries and help maintain vessel integrity, regulate permeability, and support repair. Astrocyte End-Feet (Barrier Support And Signalling) Astrocytes are support cells in the brain. Their “end-feet” surround blood vessels and help maintain BBB function through signalling and regulation. How The Blood-Brain Barrier Works Because the BBB is so selective, most substances cannot just drift into brain tissue. Entry is controlled mainly through specific routes: Passive diffusion (limited) Some small, non-charged, and fat-soluble (lipid-soluble) molecules can cross more easily by diffusion. Carrier transport (nutrients get VIP access) Essential molecules that the brain needs, but that are water-soluble, use transporters, such as: Glucose transporters (for the brain’s primary fuel) Amino acid transporters (for building blocks of proteins and neurotransmitters) Receptor-mediated transport (selective “escorts”) Certain larger molecules can cross via receptor-based mechanisms (think: a locked gate that opens for specific credentials). Efflux pumps (active “bouncers”) The BBB also has efflux transporters that pump certain substances out of brain tissue back into blood. This is a major reason many drugs struggle to reach effective levels in the brain. What Can Cross The Blood-Brain Barrier? A helpful way to think about BBB access is this: small + lipid-soluble + uncharged tends to cross more easily, while large + water-soluble + charged usually needs a transporter or cannot cross well. Common examples that may cross the BBB to some degree include: Oxygen and carbon dioxide Some anaesthetic agents Some psychiatric and anti-seizure medications Alcohol and caffeine (both can affect the brain partly because they can cross) Important note: Whether a specific medicine crosses the BBB depends on its chemical properties and how strongly it is pumped out by efflux transporters. This is why two drugs in the same category can behave differently. What Usually Cannot Cross The Blood-Brain Barrier? The BBB blocks many things that could harm the brain, including: Many bacteria and viruses (though some infections can still reach the brain through other mechanisms) Many toxins and large proteins Many antibiotics and chemotherapy agents (which is why treating brain infections and brain tumours can be challenging) What Happens When The Blood-Brain Barrier Is Disrupted? The BBB is strong, but it is not invincible. Inflammation, injury, reduced oxygen, and vascular damage can weaken barrier function. When that happens, substances that are usually kept out may leak into brain tissue, potentially triggering swelling, inflammation, and changes in brain signalling. Conditions Linked With BBB Dysfunction (High Level) BBB disruption has been associated with a range of conditions, including: Stroke (especially in the area around injured tissue) Traumatic brain injury (TBI) and concussion Meningitis and encephalitis (brain and brain-lining infections) Multiple sclerosis and other inflammatory conditions Some neurodegenerative diseases (research shows BBB changes may play a role in certain cases) Chronic metabolic and vascular stress (such as uncontrolled high blood pressure or high blood sugar, which can affect vessel health) This does not mean BBB dysfunction is the only cause of these conditions. It is better understood as one piece of a complex puzzle. BBB And Neurodegenerative Diseases BBB changes are increasingly discussed in research on neurodegenerative diseases, meaning conditions that involve progressive changes in the brain over time. In some studies, BBB dysfunction has been linked with: Reduced clearance of waste proteins from the brain Increased inflammation signalling within brain tissue Greater vulnerability of neurons to metabolic and vascular stress In practical terms, BBB dysfunction is considered a potential contributor in some cases, rather than a single “root cause.” Neurodegenerative diseases are complex, and most experts view BBB changes as one factor among genetics, immune activity, vascular health, and other brain processes. The Role Of The BBB In Cancer The BBB matters in cancer mainly because it influences how well treatments can reach brain tissue. This is relevant in two major situations: Primary brain tumours (tumours that start in the brain) Metastases (cancers that spread to the brain from elsewhere in the body) Key points clinicians and researchers consider: Drug delivery is challenging: Many chemotherapy drugs and large targeted therapies struggle to cross an intact BBB in effective amounts. The barrier can be abnormal in tumour regions: Tumours can disrupt the BBB locally, but the disruption is often uneven. Some areas may be leaky while others remain protected, which can lead to patchy drug penetration. The “blood-tumour barrier” concept: In tumours, the barrier environment may differ from normal BBB. It can still block drugs even when it appears more permeable, which complicates treatment strategies. This is why brain tumour treatment often requires carefully selected therapies and, in some cases, a combination of surgery, radiation, and drug approaches designed to improve access to the tumour. Does BBB Disruption Cause Symptoms On Its Own? Usually, BBB disruption is not something you can “feel” directly. Symptoms are more often caused by the underlying condition affecting the brain (like stroke, infection, or inflammation). However, depending on the cause and the brain areas involved, symptoms might include: Headache, fever, neck stiffness (more typical with infections) Confusion, drowsiness, or altered alertness New neurological symptoms such as weakness, speech difficulty, seizures, or severe imbalance (more concerning for urgent causes) When To Seek Urgent Medical Care Seek emergency care if someone develops sudden neurological symptoms such as: Sudden one-sided weakness or numbness Facial drooping Trouble speaking or understanding speech New seizure Severe sudden headache Severe confusion, fainting, or reduced consciousness Sudden vision loss or major balance problems These can indicate conditions like stroke, severe infection, or other time-sensitive emergencies. How Doctors Evaluate Conditions Involving The BBB Clinicians do not usually “test the BBB” as a standalone screening step. Instead, they evaluate the condition that may be affecting the brain and its vessels. History And Neurological Exam A clinician will focus on symptom timing (sudden vs gradual), triggers, fever or infection signs, medications, and risk factors (blood pressure, diabetes, immune conditions). A neurological exam checks strength, sensation, coordination, speech, eye movements, and reflexes. Imaging (Often Essential) Depending on symptoms, doctors may recommend: MRI brain: high-detail soft-tissue imaging; sometimes uses contrast to evaluate inflammation, tumours, or areas where the BBB may be more permeable CT head: often used in emergencies because it is fast, especially for bleeding concerns Lab Tests (To Identify Contributors) Blood tests depend on the clinical scenario. A clinician may recommend tests such as: Complete Blood Count (CBC) Electrolytes (sodium, potassium, calcium, magnesium) Blood glucose and or HbA1c Inflammation markers (for example, CRP, when relevant) Infection-related testing when clinically suspected In certain cases (especially suspected infection or inflammation), clinicians may recommend cerebrospinal fluid (CSF) testing via lumbar puncture, because CSF can provide important clues about inflammation and infection in and around the brain. Why The BBB Matters For Medicines The BBB is a major reason some brain conditions are hard to treat: many drugs cannot reach the brain in sufficient amounts. This shapes how medications are designed and how treatment plans are chosen. Researchers are exploring multiple strategies to improve brain drug delivery (for example, designing drugs that use existing transport systems or temporarily opening the barrier under controlled conditions). These approaches are active areas of medical research and are used only in specific settings under specialist care. How The BBB Affects Mental Health Mental health conditions are complex and involve brain circuits, neurotransmitters, hormones, immune signalling, life experience, and genetics. BBB research adds another layer: the barrier influences how inflammatory molecules, stress-related hormones, and certain signalling compounds interact with the brain. High-level ways BBB function may be relevant include: Inflammation signalling: When the BBB is disrupted, inflammatory molecules from the bloodstream may have more influence on brain tissue, which can affect mood and cognition in some contexts. Stress pathways: Chronic stress can change hormone levels and immune activity. Some research explores how stress-related signalling may interact with BBB regulation. Treatment effects: Some psychiatric medicines are effective partly because they can cross the BBB. Drug design and dosing also consider BBB transport and efflux pumps. Important note: BBB changes are not considered a standalone explanation for anxiety, depression, or other conditions. Instead, BBB research helps scientists explore why inflammation and systemic health can sometimes influence mood, sleep, and cognition. Current Breakthroughs In BBB Research BBB research is active and fast-moving. While many advances remain in specialist or research settings, several areas are shaping how scientists think about brain health and treatment: Better imaging of BBB permeability: Advanced MRI and other techniques are being used to study subtle BBB changes in living patients, helping researchers explore relationships with disease progression and symptoms. Targeted drug delivery systems: Work is ongoing on nanoparticles, engineered carriers, and “molecular Trojan horse” approaches that aim to transport medicines across the BBB more efficiently. Focus on transporters and efflux pumps: Researchers are studying how to use existing BBB transport mechanisms, or reduce drug “pumping out,” to improve medication effectiveness in the brain. Immune and vascular interactions: The neurovascular unit is being studied as a dynamic system, with attention to how immune signalling, vascular health, and BBB integrity influence brain outcomes. These advances do not mean new treatments are broadly available yet, but they explain why BBB science is a major focus in neurology and drug development. The Future Of BBB Treatments Future BBB-related treatments generally aim to do one of two things: protect the barrier when it is at risk, or safely deliver therapies across it when treating brain disease. Areas being explored include: Barrier protection strategies: Approaches that reduce inflammation, oxidative stress, or vascular injury to help preserve BBB integrity in conditions like stroke or chronic vascular disease. Controlled BBB opening: Techniques such as focused ultrasound with microbubbles are being studied to temporarily and locally open the BBB under controlled conditions to deliver medicines, especially in oncology and some neurodegenerative research contexts. Personalized drug selection: As knowledge grows about BBB transport and efflux activity, clinicians may increasingly use therapies chosen for their ability to reach brain tissue effectively. Combination approaches: In some conditions, the best results may come from combining systemic treatments, targeted delivery systems, and strategies that support vascular health. These are evolving areas of research and, in many settings, remain limited to specialized centres and clinical trials. Can You Protect Your Blood-Brain Barrier? There is no guaranteed way to “strengthen” the BBB with a supplement or quick fix. But supporting overall vascular and metabolic health helps protect the brain’s blood vessels, which indirectly supports BBB function. Practical habits include: Manage blood pressure, blood sugar, and cholesterol if your clinician advises Treat infections promptly (especially severe or spreading infections) Use helmets and seatbelts to reduce head injury risk Avoid substance misuse and follow medication guidance Prioritize sleep and recovery, since brain repair systems work best with consistent rest FAQs What Is The Blood-Brain Barrier In Simple Words? It is a protective filter in the brain’s blood vessels that controls what can enter brain tissue from the bloodstream. What Is The Main Function Of The BBB? To protect the brain and keep its chemical environment stable by allowing needed nutrients in and blocking many harmful substances. What Cells Make Up The Blood-Brain Barrier? The BBB is built mainly from tightly sealed endothelial cells, supported by a basement membrane, pericytes, and astrocyte end-feet. What Can Cross The Blood-Brain Barrier? Small lipid-soluble molecules can cross more easily, while important nutrients like glucose use specialized transporters. Some medicines can cross, but many cannot. What Prevents Toxins And Germs From Reaching The Brain? Tight junctions limit leakage between cells, and transport systems plus efflux pumps control entry and actively remove certain compounds. What Happens If The Blood-Brain Barrier Is Damaged? It can become more permeable, allowing unwanted substances and inflammatory cells into brain tissue, which may worsen swelling or inflammation depending on the cause. Is BBB Disruption Linked To Multiple Sclerosis? BBB changes are associated with inflammatory activity in multiple sclerosis, and barrier dysfunction is considered part of the disease process in many cases. Why Is The BBB A Challenge For Treating Brain Diseases? Many drugs cannot cross the BBB effectively, making it harder to deliver treatment to brain tissue. Can A Blood Test Diagnose BBB Leakage? Not reliably as a simple screening test. Doctors usually rely on clinical evaluation, imaging, and condition-specific tests (and sometimes CSF studies) depending on symptoms. How Do Doctors Check BBB-Related Problems? They evaluate the underlying condition using history, neurological exam, imaging (CT or MRI), and targeted blood or CSF tests when indicated.

Chondroma Tumors: Causes, Symptoms & Treatment Options
What is a Chondroma Tumour? A chondroma is a benign cartilaginous tumour composed of mature hyaline cartilage that develops within bone or soft tissue that develops within bones or soft tissues throughout the body. Grossly, they appear as bluish-white, glistening nodules, often with areas of calcification when examined directly. Chondromas most frequently involve the small tubular bones of the hands and feet, particularly the phalanges and metacarpals, though they can also develop in larger bones like the humerus (upper arm) or femur (thighbone). Unlike malignant Tumors, a chondroma grows slowly over months or years, often remaining undetected until symptoms appear or incidental discovery during unrelated medical examinations. Because chondromas are benign, they do not metastasize or invade adjacent soft tissues, though they can cause pressure-related symptoms to other body parts or invade vital organs. However, their growth can compress nearby structures, potentially causing significant symptoms depending on their location and size. According to a study published in Frontiers in Surgery, the age of onset for chondromas typically ranges from 20 to 60 years, with a peak incidence between 20 and 30 years. Types of Chondromas • Enchondroma: The most common type, developing within the bone marrow cavity • Periosteal chondromas: Tumors forming on the bone's outer surface or border • Juxtacortical chondromas: Another classification for surface-located Tumors • Soft tissue chondromas: Masses developing in soft tissues, particularly fingers, hands, toes, and feet • Cranial chondromas: Tumors occurring in skull base and paranasal sinuses • Pulmonary chondroma: A rare benign lung lesion sometimes associated with Carney triad (alongside gastric stromal Tumors and paragangliomas) Causes of Chondroma Tumors The exact causes of chondroma Tumors remain largely unknown to medical professionals. Unlike many other conditions where specific risk factors are well-established, chondromas appear to develop sporadically without clear predisposing factors. Most chondromas are sporadic; however, multiple lesions occur in syndromic forms such as Ollier disease (enchondromatosis) and Maffucci syndrome, which may carry a low risk of malignant transformation. They simply occur when cartilage cells begin abnormal growth patterns within bone tissue. However, certain genetic conditions like Ollier disease and Maffucci syndrome can increase the likelihood of developing multiple chondromas throughout the body. The slow-growing nature of chondromas means they may remain present for extended periods before becoming symptomatic or being discovered during unrelated medical procedures. This characteristic makes determining exact onset timing particularly challenging for doctors. Symptoms of Chondroma Tumors Chondromas often remain asymptomatic for considerable periods due to their gradual growth pattern. However, when symptoms do develop, they typically result from compression of surrounding structures. Common symptoms include: Visual disturbances or vision problems, most frequent in cranial chondromas Persistent headaches, common with skull base locations Palpable mass or noticeable bump, particularly evident in hand and foot chondromas Localised swelling around the tumour site Hearing difficulties may occur with skull base chondromas Dull, aching pain, more common in periosteal chondromas Weakness, numbness, or bowel/bladder dysfunction can occur rarely when spinal chondromas compress neural structures How is a Chondroma Diagnosed? Diagnosis begins with clinical evaluation and imaging. For cranial or spinal cases, neurological examination helps assess nerve involvement. This process helps assess cranial nerve function and overall neurological status, particularly important for skull-based Tumors. Because chondromas grow slowly and may exist asymptomatically for years, diagnosis often occurs incidentally during imaging performed for unrelated medical reasons. Your doctor will take a detailed medical history and conduct physical examinations to identify any palpable masses or neurological deficits. The combination of clinical presentation and imaging findings allows doctors to differentiate chondromas from other bone conditions and potential malignancies like chondrosarcoma. Diagnostic and Imaging Tests for Chondroma • X-rays: Reveal well-circumscribed, radiolucent lesions with possible chondroid calcifications (‘rings and arcs’ pattern), often surrounded by a thin sclerotic rim. • CT scan: Offers excellent bone detail and helps evaluate cortical integrity and matrix mineralization, bone involvement, and relationship to surrounding structures with excellent bone detail. • MRI scan: Demonstrates lobulated lesions with low-to-intermediate signal on T1 and high signal on T2, helping differentiate from chondrosarcoma, particularly valuable for assessing tumour extent and planning surgical approaches. • Bone Scans: Utilise radioactive tracers to evaluate bone metabolism and identify areas of increased activity associated with tumour growth. • Biopsy: Sometimes necessary for definitive diagnosis, involving tissue sample collection for microscopic examination to confirm chondroma characteristics. • Complete Blood Count (CBC): Routine blood tests help assess overall health status and identify any systemic conditions affecting treatment decisions. Treatment Options for Chondromas Treatment approaches vary significantly based on symptom severity, tumour location, and patient factors: • Surgical Removal: The primary treatment for symptomatic chondromas, offering potential cure through complete tumour excision. • Endoscopic endonasal approach (EEA): A minimally invasive surgical technique used for skull base chondromas, offering improved visualization and reduced morbidity, accessing through natural nasal corridors without external incisions. • Complete Excision: Traditional surgical removal through direct incision, particularly effective for accessible Tumors in hands and feet. • Watchful Waiting: Conservative monitoring approach for asymptomatic chondromas not threatening vital structures or causing functional problems. • Bone Grafting: May accompany tumour removal to replace missing bone tissue and restore structural integrity. Surgical Treatment for Chondromas Surgical removal represents the primary treatment for symptomatic chondromas. For skull base and paranasal sinus locations, specialists often prefer the endoscopic endonasal approach, a minimally invasive technique using nasal cavities as natural access corridors. This innovative approach offers significant advantages over traditional open surgery, including no external incisions, no facial disfigurement, and faster recovery times. For hand and foot lesions, intralesional curettage or excision under local or general anaesthesia is typically curative, which means scraping out the tumour under anaesthesia. After tumour removal, bone grafts may be required to replace missing bone and restore structural integrity. Non-Surgical Management of Chondromas For asymptomatic chondromas causing no functional problems, watchful waiting represents a reasonable approach. Your doctor may choose to monitor the tumour over time through periodic imaging studies, ensuring it's not growing or compressing nearby structures. This approach avoids surgical risks whilst maintaining vigilance for behavioural changes. Patients typically receive instructions to report new symptoms like pain, swelling, vision changes, or neurological symptoms, which would prompt reassessment and possible surgical intervention. Chondromas in Children vs. Adults • Age patterns: Soft tissue chondromas commonly develop during middle age, whilst periosteal types occur at any age • Location differences: Children may present with various bone locations; adults show more typical distribution patterns • Symptom recognition: Children might more readily notice palpable masses in hands and feet • Growth rates: Paediatric chondromas grow slowly over months or years • Treatment approaches: Surgical principles remain similar, though growth plate considerations may apply Prognosis for Chondroma Tumors The prognosis for chondroma Tumors is generally excellent, with most patients experiencing complete recovery after appropriate treatment. These benign Tumors rarely recur following complete surgical removal, and the risk of complications remains low when treated by experienced medical teams. Most people return to normal activities within weeks to months after surgery, depending on the tumour location and surgical approach. Long-term follow-up typically involves periodic imaging to ensure no recurrence, though this becomes less frequent over time as the risk diminishes. Chondromas and Cancer Risk Understanding chondroma cancer risk helps patients navigate their health journey with confidence. Unlike chondrosarcoma, which is malignant, chondromas remain benign throughout their existence. However, certain genetic conditions like Ollier disease and Maffucci syndrome may slightly increase the transformation risk to chondrosarcoma. The vast majority of chondromas never become cancerous, making the chondroma cancer connection relatively uncommon. Regular monitoring through clinical examinations and appropriate imaging studies helps detect any suspicious changes early, ensuring optimal outcomes for all patients. Conclusion Understanding chondroma Tumors empowers you to recognise symptoms, seek appropriate medical care, and make informed treatment decisions. While these benign cartilage Tumors can cause concerning symptoms, the prognosis remains excellent with proper diagnosis and treatment. Whether dealing with enchondroma in your hand or a cranial chondroma causing headaches, early medical consultation ensures the best outcomes. Remember that chondroma cancer transformation is rare, and most patients enjoy complete recovery after treatment. If you notice persistent lumps, unexplained pain, or neurological symptoms, don't hesitate to consult your doctor for proper evaluation. At Metropolis Healthcare, we support your diagnostic journey with comprehensive testing services. Our extensive network of over 220 laboratories and 4,600 service centres ensures accessible, accurate diagnostics when you need them most. From routine blood tests to specialised imaging support, our home sample collection service brings convenience to your doorstep across 10,000+ touchpoints nationwide. FAQs Can chondromas become cancerous? Malignant transformation of solitary chondromas is exceedingly rare; however, multiple enchondromas in Ollier disease or Maffucci syndrome carry up to a 30% risk of secondary chondrosarcoma. These benign Tumors typically remain non-cancerous throughout their existence, though regular monitoring helps detect any suspicious changes early. What are the main symptoms of a chondroma? Common symptoms include palpable masses, localised pain, swelling, and functional impairment. Cranial chondromas may cause vision problems, headaches, or hearing difficulties depending on location. How are chondromas treated? Treatment depends on symptoms and location. Symptomatic chondromas typically require surgical removal, whilst asymptomatic Tumors may be monitored through regular clinical examinations and imaging studies. Are chondromas hereditary? Chondromas aren't typically hereditary conditions. However, genetic syndromes like Ollier disease and Maffucci syndrome can increase the likelihood of developing multiple chondromas throughout the body.

Cold Urticaria: What It Is, Why It Happens & How to Manage It
What is Cold Urticaria? Cold urticaria is a type of physical urticaria in which exposure to cold air, water, or objects triggers an allergic skin reaction, causing sudden hives, redness, and swelling within minutes. The immune system mistakenly treats cold exposure as a harmful stimulus, triggering mast cells in the skin to release histamine and other inflammatory mediators that dilate blood vessels and leak fluid into surrounding tissues. While most cases are mild and self-limiting, severe reactions may involve systemic symptoms and require immediate medical care. How Cold Urticaria Affects the Body Cold urticaria sets off an inflammatory cascade when the skin encounters cold. Mast cells release histamine and other mediators, causing small blood vessels to dilate and leak fluid into the skin, leading to raised, itchy hives that usually resolve while most cases are mild and self-limiting, severe reactions may involve systemic symptoms and require immediate medical care. In severe reactions, this process can involve the lungs and cardiovascular system, triggering breathing difficulty, low blood pressure, or even anaphylaxis, which requires urgent medical care. Types of Cold Urticaria Several forms of cold urticaria exist, each with distinct features: Primary acquired cold urticaria: Most common; triggered by direct cold exposure. Secondary cold urticaria: Linked to underlying conditions like infections or blood disorders. Familial Cold Autoinflammatory Syndrome (FCAS): A rare inherited autoinflammatory disorder that causes hives, fever, and joint pain after generalized cold exposure. Cold Urticaria Symptoms Recognising cold urticaria symptoms helps you identify when you're experiencing this condition. The primary manifestations include: Rapid appearance of hives or welts after cold exposure Itching, burning, or stinging sensation Swelling of hands, face, lips, or eyelids Redness or patches on exposed skin In severe cases: breathing difficulty, dizziness, or fainting after sudden cold exposure As per the National Organisation for Rare Disorders (NORD), cold urticaria accounts for a small subset of chronic inducible urticarias and can cause rapid hives and swelling within minutes of cold exposure, with some patients experiencing systemic reactions. NORD notes that both typical and atypical forms exist, and that the condition may be primary or secondary to other diseases, though its exact cause remains unclear. Common Triggers of Cold Urticaria Any sudden drop in temperature can trigger cold urticaria. Most reactions occur when the skin warms after exposure to cold. Some common triggers include: Cold water exposure (e.g., swimming, washing hands, or being caught in rain) Cold weather or wind Prolonged exposure to air-conditioned environments Holding cold objects (ice, frozen foods, metal cans) Cold drinks or ice cream contacting the lips. Sudden temperature change from warm to cold What Causes Cold Urticaria? The exact cause of cold urticaria is unclear, but it is thought to involve abnormal mast cell activation, where cold exposure triggers histamine release and inflammation. In some people, cold may provoke an IgE-mediated autoimmune response that makes mast cells overly sensitive, while secondary cold urticaria can be linked to infections, autoimmune diseases, or blood disorders. Cold Stimulation Test (Ice Cube Test) Doctors use a simple test to diagnose cold urticaria: An ice cube is placed inside a plastic bag. The bag is applied to the skin—usually the forearm—for 1–5 minutes. After removing the ice, the skin is observed for the development of a raised, itchy wheal. A raised, red welt confirms the diagnosis of cold urticaria. When Doctors Recommend the Test This test is recommended when a person develops unexplained hives or chronic hives after cold exposure or when there is a suspected severe reaction to cold water. Complications of Cold Urticaria While many people experience mild reactions, cold urticaria can lead to serious complications: Severe allergic reaction (anaphylaxis) Difficulty breathing or shortness of breath after sudden full-body cold exposure Rapid drop in blood pressure Fainting episodes Swelling of the throat or tongue Danger during cold-water swimming or diving Cold Urticaria Treatment Options Effective cold urticaria treatment focuses on symptom management and prevention. Treatment approaches include: Antihistamines: The first-line treatment to reduce hives and itching. Leukotriene modifiers: For people who don’t respond to antihistamines. Omalizumab: Used in chronic or severe cases. Emergency epinephrine: For patients with a history of severe reactions. Avoiding known triggers and maintaining warmth: Key components of long-term management. Home Remedies & Self-Care Tips for Cold Urticaria Managing cold urticaria involves practical strategies to minimise exposure and reduce symptom severity. Daily Precautions Dress in layers during winter. Use gloves, scarves, and face coverings. Warm the car before stepping outside to reduce cold shock. Avoid sudden exposure to cold water. Lifestyle & Prevention Tips Test the water temperature with your hand before bathing. Avoid ice-cold drinks if lip swelling occurs. Carry prescribed antihistamines (and an epinephrine auto-injector if advised) when travelling. Inform swimming instructors or companions about your condition. When to See a Doctor? Seek medical help if symptoms occur frequently or if hives appear without clear triggers. Immediate care is needed if cold exposure leads to: Difficulty breathing Fainting Swelling of the throat Severe dizziness or low blood pressure How Cold Urticaria is Diagnosed Healthcare providers use a systematic approach to diagnose cold urticaria: Detailed medical history Ice cube test Physical examination Laboratory tests to rule out secondary causes Allergy evaluation, if needed Tests for Cold Urticaria ABPA Panel Test: Blood panel to assess allergy to Aspergillus in patients with asthma-like or respiratory symptoms. Alternaria Alternata (Specific IgG): Checks IgG antibodies to Alternaria mould linked with environmental allergy. Aspergillus fumigatus(Specific IgG): Measures IgG to A. fumigatus to assess possible mould-related allergy. Allergen, Individual-Microorganism Cladosporium Herbarum fungus: Evaluates IgE response to circulating allergen-specific IgE for Cladosporium herbarum (Fungus). Allergen, Individual-Microorganism Penicillium Notatum fungus (Penicillium chrysogenum): Screens for specific IgE antibodies to Penicillium mould as part of allergy workup. Medical History Evaluation Doctors ask about symptoms, exposure patterns, family history, and past allergic conditions. Physical Exam & Lab Tests During physical examination, your doctor assesses your skin condition, checks for signs of other allergic diseases, and evaluates your overall health status. Laboratory tests may include: CBC (Complete Blood Count) Test Thyroid Profile Test (TFT) Autoimmune screening (e.g., ANA test) to detect possible systemic causes Tests for infections with an Opportunistic Infection Panel Screening for chronic hives or associated disorders Cold Urticaria in Children: What Parents Should Know Cold urticaria can affect children, requiring special considerations for management and safety. Parents should watch for symptoms after cold exposure and teach children to recognise early warning signs. Children may experience more intense or unpredictable reactions to cold exposure. Swelling around the lips or hands after ice cream is common. Avoid swimming in cold water unless a doctor clears it. Keep emergency medication handy in case of severe reactions. Most children outgrow cold urticaria within a few years, though monitoring is advised. Cold Urticaria Outlook & Long-Term Management The outlook for cold urticaria differs from person to person. Many improve over time, and some go into complete remission within a few years, while others may have symptoms for longer and need ongoing management. With the right treatment, trigger avoidance, and regular medical follow-up, most people can maintain a good quality of life and continue normal activities with sensible precautions. Conclusion Cold urticaria can usually be well managed with proper diagnosis, preventive care, and ongoing treatment where needed. Recognising your triggers early and consulting a doctor if reactions are frequent or severe helps prevent complications and supports safer day-to-day living. As a trusted diagnostic partner, Metropolis Healthcare offers 4,000+ tests, full-body checkups, specialised allergy and immunology testing, and strong home sample collection across 10,000+ touchpoints, with quick turnaround and accurate results. You can book tests conveniently via website, app, WhatsApp, or phone, making it easier to get timely, reliable reports that support your doctor in managing cold urticaria effectively. FAQs What triggers cold urticaria the most? The most common triggers include sudden exposure to cold air, cold water, cold wind, and contact with cold objects. Swimming in cold water is among the strongest triggers due to the rapid temperature drop. Can cold urticaria be cured permanently? There is no permanent cure, but symptoms can be effectively controlled. Many people with primary cold urticaria improve over 5–10 years. Is cold urticaria a serious condition? It can be serious if it triggers whole-body reactions, such as fainting or breathing difficulties, especially after swimming. Most cases are mild but require caution. How long does a cold urticaria reaction last? Localised reactions usually last 1–2 hours. More severe reactions may last longer and require medical attention. Can you swim if you have cold urticaria? Swimming should be avoided in cold water. If approved by a doctor, warm-water swimming may be safe under supervision. What foods should be avoided with cold urticaria? Ice-cold drinks Ice cream, if it triggers lip swelling Frozen foods that require handling

Movement Disorders: Types, Symptoms & When to Seek Help
What are Movement Disorders? Movement disorders are a group of neurological conditions that affect your body's ability to produce and control normal movement patterns. These conditions originate in the nervous system, specifically disrupting the brain regions responsible for coordinating muscle activity and movement control. Movement disorders can manifest as either reduced movement (hypokinetic conditions like Parkinson's disease) or excessive, uncontrolled movement (hyperkinetic conditions such as essential tremor, chorea, or other involuntary movements). More than 30 different diseases are classified as movement disorders, with symptoms varying widely among individuals but often progressing over time. How the Nervous System Controls Movement Your nervous system orchestrates all voluntary and involuntary movements through an intricate network of neural pathways connecting your brain, spinal cord, and muscles. The brain sends precise signals through the spinal cord to peripheral nerves, instructing muscles when to contract and relax in coordinated patterns. Movement disorders occur when disruptions affect these neural communication pathways. The sensorimotor cortex, basal ganglia, and cerebellum play crucial roles in movement coordination. When damage or dysfunction occurs in these brain regions, it leads to the characteristic abnormal movement patterns seen in various movement disorders. This disruption can stem from genetic factors, neurodegeneration, or environmental influences affecting how your brain processes and executes movement commands. Types of Movement Disorders Understanding different movement disorder types helps recognise symptoms and seek appropriate treatment: Parkinson's disease: A progressive neurological condition causing tremors, muscle rigidity, slowness of movement, and balance problems. Essential tremor: Involuntary rhythmic shaking, primarily affecting hands and neck during voluntary movement. Dystonia: Sustained muscle contractions causing repetitive, twisting movements and abnormal postures. Huntington's disease: Inherited disorder characterised by chorea (irregular, dance-like movements) and cognitive decline. Tourette syndrome: A neurological condition involving repetitive movements and vocal sounds called tics. Ataxia: A degenerative disorder affecting coordination, balance, and speech. Myoclonus: Sudden, brief muscle jerks or twitches. Restless legs syndrome: Uncomfortable leg sensations creating an urge to move. Multiple system atrophy: A rare condition affecting movement, blood pressure, and bladder control. Progressive supranuclear palsy: A rare neurodegenerative disorder affecting walking, balance, and eye movement control. Common Symptoms of Movement Disorders Movement disorders' symptoms vary depending on the specific condition, but several key indicators warrant attention: Tremors or involuntary shaking movements, especially at rest or during activity. Muscle rigidity or stiffness that affects normal movement. Bradykinesia (abnormally slow movement). Difficulty walking or noticeable changes in gait patterns. Loss of balance and coordination problems. Involuntary muscle contractions or spasms. Jerky, irregular movements affecting arms, legs, or the entire body. Speech difficulties or voice changes. Excessive fidgeting or inability to remain still. Facial grimacing or unusual expressions. Problems with fine motor skills, like writing or buttoning clothes. Are you experiencing unusual movements that interfere with daily activities? Early recognition of movement disorder symptoms can lead to timely intervention and better outcomes. What Causes Movement Disorders? Movement disorders' causes are diverse and often complex, involving multiple factors: Genetic mutations: Inherited conditions like Huntington's disease result from specific gene defects. Neurodegeneration: Progressive damage to brain cells, particularly in areas controlling movement. Neurotransmitter imbalances: Disruption in chemical communication between brain cells. Environmental toxins: Exposure to certain chemicals or heavy metals. Brain injuries: Trauma affecting movement-controlling brain regions. Infections: Viral or bacterial infections affecting the nervous system. Medication side effects: Certain drugs can trigger movement abnormalities. Autoimmune conditions: Immune system attacks on components of the nervous system. Risk Factors You Should Know Understanding movement disorders causes helps healthcare providers develop targeted treatment approaches and may inform prevention strategies for at-risk individuals. Several factors can increase your likelihood of developing movement disorders: Age: Many movement disorders become more common with advancing age, particularly after 60. Family history: A genetic predisposition significantly increases the risk of inherited conditions. Gender: Some conditions show gender preferences; for example, men develop Parkinson's disease more frequently. Environmental exposure: Occupational or residential exposure to pesticides, heavy metals, or industrial solvents. Previous head injuries: Traumatic brain injuries may increase susceptibility to certain movement disorders. Medication history: Long-term use of certain psychiatric or antiemetic medications. Possible Complications Without proper management, movement disorders can lead to serious complications: Progressive decline in mobility and independence Increased fall risk and potential injuries Speech and swallowing difficulties (dysarthria and dysphagia) Cognitive impairment and dementia Depression and anxiety disorders Social withdrawal and isolation Sleep disturbances, including insomnia or excessive daytime sleepiness Nutritional problems due to eating difficulties Respiratory complications from swallowing issues Reduced quality of life for patients and families How Movement Disorders Are Diagnosed Healthcare providers use a systematic approach to diagnose movement disorders: Comprehensive medical history: A detailed discussion of symptoms, family history, medications, and potential environmental exposures. Neurological examination: Assessment of reflexes, muscle strength, coordination, gait, and movement patterns. Symptom observation: Careful evaluation of abnormal movements during rest and activity. Cognitive assessment: Testing memory, thinking skills, and mental function. Differential diagnosis: Ruling out other conditions that might mimic movement disorders. Tests for Movement Disorders Diagnostic testing helps confirm movement disorders and guide treatment decisions: Brain imaging: MRI or CT scans to identify structural abnormalities. Blood tests: Comprehensive metabolic panel to assess overall health. Autoimmune Parkinsonian Profile: Specialised testing for immune-related movement disorders. Huntington disease mutation analysis: Specific genetic test for Huntington's disease. Gene panels: Genetic screening for various dystonia types or specific conditions, such as the Early-Onset Juvenile Parkinsonism Gene Panel. Cerebrospinal fluid analysis: Examination of spinal fluid when indicated, with tests like the Bacterial Meningitis Panel, CSF. Electromyography (EMG): Testing muscle and nerve function. Treatment Options for Movement Disorders Movement disorders treatment varies based on the specific condition and severity: Medications: Dopamine replacement therapy, muscle relaxants, anticonvulsants, and botulinum toxin injections. Deep brain stimulation: Surgical implantation of electrodes to regulate abnormal brain activity. Physical therapy: Exercises to improve strength, flexibility, balance, and coordination. Occupational therapy: Strategies to maintain independence in daily activities. Speech therapy: Techniques to address communication and swallowing difficulties. Lifestyle modifications: Regular exercise, stress management, and adequate sleep. Support groups: Peer support and education for patients and families. Lifestyle Tips to Manage Movement Disorders Daily management strategies can significantly improve quality of life: Maintain regular exercise routines appropriate for your condition. Follow a balanced, nutritious diet rich in antioxidants. Establish consistent sleep schedules and good sleep hygiene. Practice stress-reduction techniques such as meditation or yoga. Use assistive devices when needed for safety and independence. Stay socially connected with family and friends. Attend regular medical appointments and follow treatment plans. Keep a symptom diary to track changes and medication effects. When to Seek Medical Help Recognising when to consult healthcare providers is crucial for optimal outcomes. Seek immediate medical attention if you experience a sudden onset of involuntary movements, severe muscle spasms, difficulty swallowing, or significant changes in existing symptoms. Early consultation allows for prompt diagnosis and treatment initiation, potentially slowing disease progression and improving long-term prognosis. Don’t wait—if movement symptoms interfere with daily activities, affect your safety, or cause emotional distress, seek evaluation promptly. Healthcare providers can offer comprehensive evaluations and develop personalised treatment plans that address your specific needs and concerns. Living With Movement Disorders: Coping & Support Living with movement disorders requires ongoing adaptation and support from healthcare teams, family, and community resources. Focus on maintaining realistic goals, celebrating small achievements, and adapting activities to accommodate changing abilities. Join support groups to connect with others facing similar challenges, share experiences, and learn practical coping strategies. Remember that movement disorders affect each person differently, and treatment responses vary. Work closely with your healthcare team to optimise treatment approaches, manage symptoms effectively, and maintain the best possible quality of life throughout your journey. Conclusion The Movement disorder treatment focuses on controlling symptoms in the past 25 years, underscoring how movement disorders as a whole are becoming an increasingly important public health concern. While these conditions can be challenging, many are manageable with timely diagnosis, appropriate medical care, lifestyle changes, and the right support systems. Recognizing early signs—such as tremors, stiffness, slowed movements, or other unusual motor symptoms—can lead to earlier intervention and improved outcomes. Whether you’re trying to understand the causes, exploring treatment options, or supporting a loved one, comprehensive and coordinated care plays a crucial role. At Metropolis Healthcare, we are committed to supporting your diagnostic journey with more than 4,000 tests, including specialised panels designed for autoimmune conditions. With 220+ laboratories and over 10,000 touchpoints across India, we ensure reliable and accessible testing whenever you need it. From genetic assessments to advanced metabolic panels, our home sample collection service delivers trusted diagnostics and convenience right to your doorstep. FAQs What are the early signs of a movement disorder? Early movement disorder symptoms often include subtle tremors, slight stiffness, balance problems, or changes in handwriting. You might notice difficulty with fine motor tasks, occasional muscle spasms, or mild coordination problems. These symptoms typically develop gradually and may initially be dismissed as normal ageing or stress-related issues. Can movement disorders be cured? Currently, most movement disorders cannot be completely cured, but many can be effectively managed with appropriate treatment. Movement disorder treatment focuses on controlling symptoms, slowing progression, and maintaining quality of life through medications, therapies, and lifestyle modifications. Early intervention often leads to better long-term outcomes. What is the most common movement disorder? Essential tremor is the most common movement disorder, affecting approximately 1% of the population worldwide. Parkinson's disease is the second most common, with over 8.5 million people affected globally according to WHO estimates. Both conditions significantly impact daily functioning but respond well to appropriate treatment approaches. Are movement disorders hereditary? Some movement disorders have genetic components, particularly Huntington's disease, certain types of dystonia, and some forms of Parkinson's disease. However, many movement disorders result from complex interactions between genetic predisposition and environmental factors. Genetic counselling can help assess your risk if you have a family history of these neurological conditions. Is Parkinson's a movement disorder? Yes, Parkinson's disease is one of the most well-known movement disorder types. It affects the brain's ability to produce dopamine, leading to characteristic symptoms, including tremors, rigidity, bradykinesia, and balance problems. The WHO reports that Parkinson's disease prevalence has doubled in the past 25 years, emphasising the importance of awareness and early detection. How do doctors diagnose movement disorders? Healthcare providers diagnose movement disorders through comprehensive neurological examinations, detailed medical histories, and observation of movement patterns. Diagnostic testing may include brain imaging, genetic analysis, blood tests, and specialised panels. The diagnostic process requires careful evaluation to distinguish between different movement disorder types and develop appropriate treatment plans. Can stress cause involuntary movements? Stress can trigger or worsen certain types of involuntary movements, including tics, tremors, and muscle spasms. However, stress alone rarely causes primary movement disorders. Chronic stress may exacerbate existing neurological conditions or contribute to functional movement disorders. Managing stress through relaxation techniques, exercise, and adequate sleep can help reduce symptom severity. Which doctor should I consult for movement disorders? Start with your primary care physician, who can perform initial assessments and provide referrals to neurologists specialising in movement disorders. Movement disorder specialists have additional training in diagnosing and treating these complex neurological conditions. They can offer comprehensive evaluation, advanced treatment options, and ongoing management strategies tailored to your specific condition.