


Preventive Healthcare
Breast Cancer Medications: Types, How They Work, And What To Expect
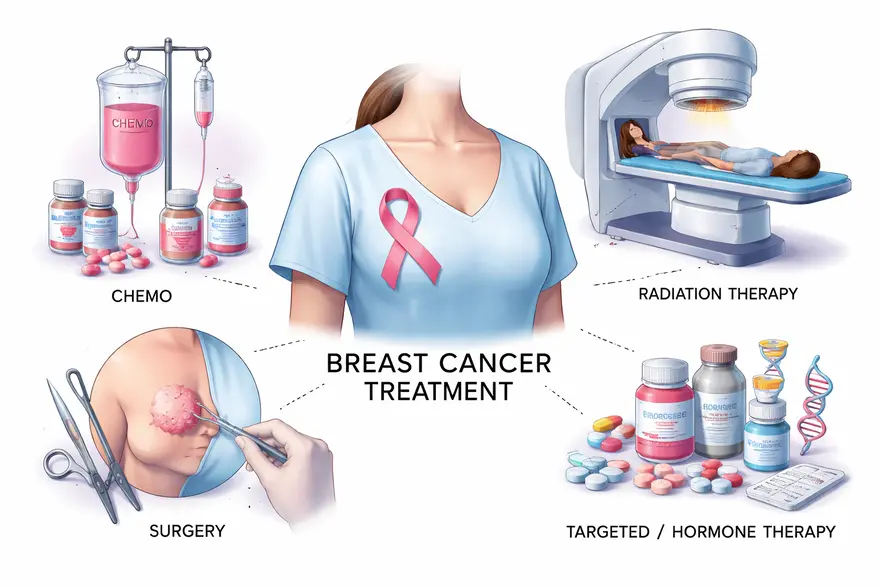
Table of Contents
- Key Takeaways
- Breast Cancer Medication
- Understanding Breast Cancer Type And Stage
- Types Of Breast Cancer Medications
- How Breast Cancer Medications Work
- How Doctors Choose The Right Breast Cancer Medication For You
- Tests That Guide Breast Cancer Medication Choices
- Benefits Of Early And Appropriate Medication In Breast Cancer
- Common Side Effects Of Breast Cancer Medications
- Managing Side Effects And Staying Comfortable During Treatment
- Taking Your Medicines Safely
- Frequently Asked Questions
- How Metropolis Healthcare Can Support You
- Conclusion
- References
Breast cancer medications include chemotherapy, targeted therapy, hormone therapy, immunotherapy, and antibody drug conjugates. Your doctor chooses these medicines based on your tumour’s characteristics, such as whether it is HER2 positive, hormone receptor positive (ER and or PR positive), or triple negative, as well as the stage and your overall health.
You may receive one medicine or a combination. In many treatment plans, medicines are combined to improve effectiveness or given in a planned sequence over time. This guide explains the main medication types, how they work, the tests that help guide treatment choices, and what side effects you may experience and manage.
Key Takeaways
- Breast cancer medicines fall into a few main groups: hormone therapy, targeted therapy, chemotherapy, immunotherapy, and antibody drug conjugates.
- Your doctor selects medicines using tumour markers like ER, PR, and HER2, plus factors such as stage and menopausal status.
- Many treatment plans use combination therapy or step-by-step sequencing to improve results and reduce the risk of recurrence.
- Most side effects can be prevented or managed with supportive care, monitoring, and timely medical advice.
Breast Cancer Medication
Breast cancer medication refers to drugs used to treat breast cancer, lower the chance of it coming back, or in some situations reduce risk in people at high risk. Medicines may be used:
- Before surgery (neoadjuvant therapy) to shrink the tumour and assess response
- After surgery (adjuvant therapy) to reduce recurrence risk
- For advanced or metastatic breast cancer to control disease and support quality of life
WHO reports that breast cancer caused an estimated 670,000 deaths globally in 2022 and that breast cancer occurs in every country in the world.
Understanding Breast Cancer Type And Stage
Why Subtype Matters
Your treatment depends heavily on tumour biology. The most common labels you may hear are:
- Hormone Receptor Positive (ER and or PR positive)
The cancer cells use hormones (oestrogen and or progesterone) as “fuel”. - HER2 Positive
The cancer cells have higher levels of a growth signal called HER2. - Triple Negative Breast Cancer (TNBC)
The tumour is ER negative, PR negative, and HER2 negative. Treatment often relies more on chemotherapy, and sometimes immunotherapy, depending on your situation.
How Stage Influences Treatment
Stage reflects tumour size and spread. Early-stage treatment often aims to cure and prevent recurrence. Advanced-stage treatment focuses on controlling cancer and preserving day-to-day wellbeing. Your doctor may also consider whether medicines should come before or after surgery, and whether radiotherapy is part of the plan.
Types Of Breast Cancer Medications
Hormone Therapy
Hormone therapy (also called endocrine therapy) is used when the cancer is hormone receptor positive.
Common examples include:
- Tamoxifen
- Aromatase inhibitors such as letrozole, anastrozole, and exemestane
- Fulvestrant (used in specific settings)
- Ovarian suppression medicines in selected premenopausal patients (your oncologist will advise)
These treatments can be highly effective for ER-positive breast cancer. Large patient-level analyses show meaningful reductions in recurrence and mortality with endocrine therapy.
Targeted Therapy
Targeted treatments focus on specific features of cancer cells. Many require biomarker testing.
HER2-targeted therapy (for HER2-positive breast cancer) may include:
- trastuzumab (Herceptin)
- pertuzumab (Perjeta)
- tucatinib (Tukysa)
- neratinib (Nerlynx)
Trials have shown that adding trastuzumab to treatment improves outcomes in HER2-positive breast cancer.
CDK4/6 inhibitors (commonly used for HR-positive, HER2-negative advanced breast cancer, often with hormone therapy):
- palbociclib (Ibrance)
- ribociclib (Kisqali)
- abemaciclib (Verzenio)
These drugs help slow cancer cell division and are typically combined with endocrine therapy.
PARP inhibitors (for eligible patients, often linked to inherited BRCA mutations):
- olaparib (Lynparza)
- talazoparib (Talzenna)
For high-risk early breast cancer with BRCA1 or BRCA2 mutations, a year of adjuvant olaparib has been shown to reduce recurrence risk.
Chemotherapy
Chemotherapy kills fast-growing cells and is used in many breast cancer settings, especially:
- Triple negative breast cancer
- Higher-risk early breast cancer
- HER2-positive breast cancer (often alongside targeted therapy)
- Advanced breast cancer
Examples include paclitaxel, docetaxel, doxorubicin, cyclophosphamide, capecitabine, and others. Your regimen depends on tumour biology, stage, and health factors.
Immunotherapy
Immunotherapy helps your immune system recognise and attack cancer. It is not used for every breast cancer type.
One example is pembrolizumab (Keytruda), used in selected triple negative breast cancer settings. A key trial in early triple negative breast cancer showed benefit when pembrolizumab was added to neoadjuvant chemotherapy and continued after surgery.
Antibody Drug Conjugates
Antibody drug conjugates (ADCs) deliver a chemotherapy payload directly to cancer cells through a targeted antibody.
Examples include:
- ado-trastuzumab emtansine (Kadcyla, also called T-DM1)
- trastuzumab deruxtecan (Enhertu, also called T-DXd)
- sacituzumab govitecan (Trodelvy)
In HER2-positive metastatic breast cancer, trastuzumab deruxtecan has shown improved outcomes compared with trastuzumab emtansine in a major randomised trial.
Medicines Used For Risk Reduction In High Risk Individuals
If you are at increased risk of breast cancer, your clinician may discuss “chemoprevention”, meaning medication to reduce risk. This is a specialist decision based on your risk profile and medical history.
Evidence from large prevention trials supports risk reduction with tamoxifen in selected high-risk women, and raloxifene as an option in postmenopausal women.
How Breast Cancer Medications Work
Blocking Hormones That Fuel Cancer Growth
Hormone therapies reduce oestrogen’s effects or lower oestrogen levels, depriving hormone receptor-positive cancer cells of growth signals.
Targeting Growth Signals And Cancer Pathways
HER2-targeted treatments block HER2 signalling, while CDK4/6 inhibitors slow cell cycle progression.
Killing Fast Growing Cells
Chemotherapy affects fast-growing cells, including cancer cells. This is why it can also affect hair follicles and bone marrow.
Helping Your Immune System Recognise Cancer
Checkpoint inhibitors like pembrolizumab help immune cells stay active against cancer in selected cases.
Delivering Treatment Directly Into Cancer Cells
ADCs link a targeted antibody to a chemotherapy payload so treatment is delivered more directly to cancer cells.
How Doctors Choose The Right Breast Cancer Medication For You
Your oncologist considers multiple factors, including:
- ER, PR, and HER2 status
- Stage and whether lymph nodes are involved
- Menopausal status and overall health
- Past treatments and how the cancer responded
- Your preferences and practical priorities, such as daily tablets versus hospital infusions
You may receive:
- Combination therapy (for example endocrine therapy plus a CDK4/6 inhibitor)
- Sequential therapy where medicines change over time depending on response, side effects, or recurrence risk
This approach is normal and is designed to keep treatment both effective and sustainable.
Tests That Guide Breast Cancer Medication Choices
Accurate testing is central to choosing the right medicines.
Tests On Your Biopsy Sample
Your biopsy report typically includes:
- Tumour type and grade
- ER and PR status
- HER2 status
- Sometimes Ki-67 (a marker related to cell growth rate)
ICMR’s Standard Treatment Workflow for breast cancer recommends testing ER, PR, HER2/neu, and Ki-67, and using FISH when HER2 is equivocal on IHC.
Biomarker And Genetic Testing That May Influence Treatment
Depending on your clinical scenario, your doctor may suggest:
- Inherited mutation testing such as BRCA1 and BRCA2
- Tumour mutation testing (for example PIK3CA in selected cases)
- PD-L1 testing in some triple negative breast cancers (to guide immunotherapy decisions)
Baseline And Monitoring Tests During Treatment
Many treatments require monitoring to keep you safe and comfortable, such as:
- Full blood count (to monitor white cells, haemoglobin, platelets)
- Liver and kidney function tests
- Glucose and lipids for certain targeted therapies
- Heart function monitoring when using therapies that can affect the heart, such as anthracyclines and HER2-targeted therapy
ASCO guidance recommends assessing and monitoring heart function in people receiving cancer therapies that may affect the heart, especially when risk factors are present.
Benefits Of Early And Appropriate Medication In Breast Cancer
Starting the right medication at the right time can:
- Reduce the risk of recurrence after surgery
- Shrink tumours before surgery, sometimes allowing less extensive procedures
- Improve control and quality of life in advanced disease
For HER2-positive breast cancer, HER2-targeted therapy added to standard treatment has shown clear benefits in clinical trials.
Common Side Effects Of Breast Cancer Medications
Side effects vary by medication and by person. You may experience none, a few, or more than expected. The aim is always to treat cancer effectively while supporting you through side effects.
Side Effects Of Chemotherapy
Common effects may include:
- Tiredness and weakness
- Nausea and appetite changes
- Hair loss (with some regimens)
- Mouth sores
- Lowered blood counts, which can increase infection risk
Side Effects Of Hormone Therapy
Possible effects include:
- Hot flushes and night sweats
- Joint and muscle aches (especially with aromatase inhibitors)
- Vaginal dryness
- Changes in mood or sleep
- Rare risks such as blood clots with tamoxifen (your doctor will assess your risk)
Side Effects Of Targeted Therapy
These depend on the drug:
- HER2-targeted therapy can sometimes affect heart function, which is why monitoring is often recommended.
- CDK4/6 inhibitors can lower white blood cells and may cause fatigue or diarrhoea, so regular blood tests are common.
Side Effects Of Immunotherapy
Immunotherapy can cause inflammation in healthy tissues because it activates the immune system. Your doctor will explain what to watch for and when to seek advice.
Side Effects Of Antibody Drug Conjugates
ADCs can cause nausea, fatigue, and low blood counts. Some ADCs have specific side effects your team will monitor for, and early reporting of symptoms is important.
Managing Side Effects And Staying Comfortable During Treatment
Practical Tips You Can Try At Home
- Eat small, frequent meals if nausea or poor appetite is an issue
- Stay hydrated and rest when you need to
- Use gentle oral care to reduce mouth soreness
- Keep a simple symptom diary so you can describe patterns clearly to your doctor
- Ask about safe physical activity, as gentle movement can help fatigue and mood
Supportive Medicines Your Doctor May Prescribe
Supportive care can make a big difference, for example:
- Anti-sickness medicines
- Medicines for diarrhoea or constipation
- Treatments for hot flushes or sleep
- Bone health support in selected patients
When You Should Contact Your Doctor Urgently
Seek prompt medical advice if you have:
- Fever or chills during chemotherapy
- Severe diarrhoea or vomiting
- New breathlessness, chest pain, or fainting
- Unusual bleeding or bruising
- A rapidly worsening rash
You are not “bothering” your team by calling. Early support is often the easiest way to prevent complications.
Taking Your Medicines Safely
- Take medicines exactly as prescribed, and do not stop suddenly unless your clinician advises it.
- Tell your doctor about supplements, herbal products, and over-the-counter medicines, as interactions can matter.
- If you miss a dose, follow your prescription guidance or ask your care team rather than doubling up.
- Discuss contraception and pregnancy planning early, because some medicines can harm a developing baby.
Frequently Asked Questions
What Are The Side Effects Of Chemotherapy For Breast Cancer?
Common side effects include tiredness, nausea, hair loss (with some regimens), mouth sores, and lowered blood counts. Not everyone experiences the same effects, and most can be managed with supportive medicines and monitoring.
What Is The Difference Between Hormone Therapy And Chemotherapy For Breast Cancer?
Hormone therapy works by blocking oestrogen’s effects or reducing oestrogen levels and is used when the cancer is hormone receptor positive. Chemotherapy attacks fast-growing cells and is used across several breast cancer subtypes, especially when the cancer is higher risk or hormone therapy alone is not enough.
How Long Do Side Effects Of Breast Cancer Medication Last?
Some side effects are short-term and improve after treatment cycles end, such as nausea or low blood counts from chemotherapy. Others can continue while you are taking long-term medicines such as hormone therapy. If a side effect is affecting your day-to-day life, tell your doctor early, because adjustments and supportive care are often available.
Do All Breast Cancers Need Chemotherapy?
No. Some breast cancers are treated primarily with surgery and hormone therapy, with or without targeted therapy, depending on the tumour subtype and recurrence risk. Your oncologist will explain why chemotherapy is recommended or not recommended in your case.
Why Do You Need ER, PR, And HER2 Testing Before Treatment?
These markers help identify which medicines are most likely to work. For example, ER-positive cancers often respond well to hormone therapy, and HER2-positive cancers may benefit from HER2-targeted medicines.
Can Medicines Help Prevent Breast Cancer If You Are High Risk?
In selected high-risk individuals, medicines such as tamoxifen or raloxifene can reduce the risk of developing invasive breast cancer. This decision should be made with a clinician after weighing benefits and risks.
How Long Will You Need To Take Hormone Therapy?
Many people take endocrine therapy for several years. Your oncologist will individualise duration based on your recurrence risk, menopausal status, and how well you tolerate treatment.
Can You Continue Working During Treatment?
Many people can, but you may need adjustments. Fatigue and appointment schedules can be challenging. It can help to plan for flexible hours, accept support, and speak to your team about symptom control.
How Metropolis Healthcare Can Support You
When your doctor recommends breast cancer testing, reliable results matter because they guide treatment decisions. Metropolis Healthcare supports you with a wide range of diagnostic services, including speciality testing aligned to oncology pathways.
With NABL and CAP-accredited labs, 4,000+ tests, and full body checkups, Metropolis Healthcare helps make testing accessible and dependable. You can also choose home sample collection, supported by a strong home collection network with 10,000 touchpoints, along with quick turnaround and accurate results. Booking is designed to be convenient through the website, app, call, and WhatsApp. In addition to supporting your testing needs, you can explore more Metropolis articles to stay informed and feel more confident in discussions with your care team.
Conclusion
Breast cancer medications can include hormone therapy, targeted therapy, chemotherapy, immunotherapy, and antibody drug conjugates. Your treatment is chosen based on your tumour’s markers, stage, and your overall health, and it is normal for plans to involve combinations or step-by-step changes over time. If you feel anxious about side effects or decisions, bring those concerns to your doctor early. You deserve clear answers and practical support throughout treatment.
References
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Davies C., Godwin J., Gray R., et al. (2011). Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level meta-analysis of randomised trials. Lancet, 378(9793), 771–784. PMID: 21802721
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). (2015). Aromatase inhibitors versus tamoxifen in early breast cancer: Patient-level meta-analysis of the randomised trials. Lancet, 386(10001), 1341–1352. PMID: 26211827
- Piccart-Gebhart M. J., Procter M., Leyland-Jones B., et al. (2005). Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. New England Journal of Medicine, 353(16), 1659–1672. PMID: 16236737
- Romond E. H., Perez E. A., Bryant J., et al. (2005). Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. New England Journal of Medicine, 353(16), 1673–1684. PMID: 16236738
- Finn R. S., Martin M., Rugo H. S., et al. (2016). Palbociclib and letrozole in advanced breast cancer. New England Journal of Medicine, 375(20), 1925–1936. PMID: 27959613
- Hortobagyi G. N., Stemmer S. M., Burris H. A., et al. (2016). Ribociclib as first-line therapy for HR-positive, advanced breast cancer. New England Journal of Medicine, 375(18), 1738–1748. PMID: 27717303
- Schmid P., Cortes J., Pusztai L., et al. (2020). Pembrolizumab for early triple-negative breast cancer. New England Journal of Medicine, 382(9), 810–821. PMID: 32101663
- Cortés J., Kim S. B., Chung W. P., et al. (2022). Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. New England Journal of Medicine, 386(12), 1143–1154. PMID: 35320644













































